
Cancer treatment has always been a major challenge in the medical field, and identifying the most effective anticancer drugs for patients is a critical part of this effort. Today, we introduce a technology that could bring a significant breakthrough to cancer treatment: the CTC drug susceptibility test.
Q1: What is the CTC drug susceptibility test?
Circulating Tumor Cells (CTCs) are tumor cells that detach from the primary tumor or metastatic sites and enter the bloodstream directly during tumor development and progression. They are a key factor in the recurrence and distant metastasis of malignant tumors.
The CTC drug susceptibility test involves isolating circulating tumor cells from a patient's blood sample and testing them in vitro with different anticancer drugs to determine which drug is most effective against the tumor. This test helps doctors select the most suitable medication for the patient, enabling more targeted treatment, avoiding wasted time and money on ineffective drugs, and reducing unnecessary side effects. If a patient has developed resistance to certain drugs, this test can also help identify new treatment options to overcome that resistance.
Q2: What is the difference and advantage of CTC-based drug susceptibility testing compared to solid tumor tissue-based testing?
CTC-based drug susceptibility testing requires only a peripheral blood sample or other bodily fluids, making it a minimally invasive procedure. Compared to traditional tumor biopsy, collecting peripheral blood causes less physical trauma and discomfort to the patient, making it more acceptable. This is especially a better option for patients who cannot undergo surgical biopsy or are in poor physical condition.
Recent studies [1] have shown that the sensitivity of drug test results based on solid tumor tissue is inferior to that of CTCs, and drug susceptibility testing based on in vitro cultured CTCs is more representative. Tissue biopsies typically capture only local information from a tumor, whereas CTCs originate from different parts of the tumor, providing a more comprehensive reflection of tumor heterogeneity.
Q3: Are there real-world examples of drug susceptibility testing? Do the test results align with pathological findings?
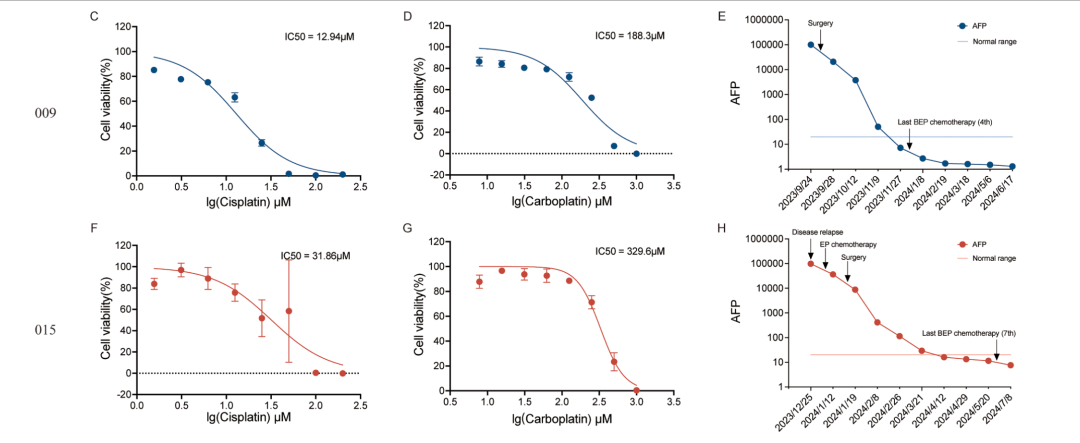
We performed drug susceptibility testing on tumor cells cultured in vitro from two patients with ovarian malignant germ cell tumors (Case NO.009, newly diagnosed; Case NO.015, recurrent). We found that cisplatin exhibited a significant inhibitory effect on tumor cell proliferation in both patients, while the inhibitory effect of carboplatin was relatively weaker.
Notably, the in vitro drug susceptibility results were highly consistent with changes in the patients' serum alpha-fetoprotein (AFP) levels. For example, the rapid decline in AFP levels in Case NO.009 corresponded to the high drug sensitivity of her cell line. This finding demonstrated for the first time that drug susceptibility results from in vitro cultured, sorted cell lines from this rare tumor can effectively predict clinical treatment response, providing an important experimental basis for personalized precision treatment of ovarian malignant germ cell tumors.
Q4: What requirements do tumor drug susceptibility tests have for drugs? Can all drugs be tested?
Tumor drug susceptibility tests have specific requirements for drugs, and not all drugs are suitable for such testing. Drugs currently amenable to in vitro drug susceptibility testing primarily include traditional chemotherapeutic agents (e.g., platinum compounds, antimetabolites, taxanes), targeted therapies (e.g., kinase inhibitors), antibody-drug conjugates (ADCs), and novel protein degraders (e.g., PROTACs). These drugs act directly on tumor cells or specific targets, and their effects can be quantitatively measured under in vitro culture conditions, making them suitable for various drug susceptibility testing methods.
However, immunotherapies (e.g., CAR-T cell therapy), hormonal therapies (e.g., tamoxifen), anti-angiogenic agents (e.g., bevacizumab), and radiotherapy rely on systemic immune modulation, in vivo metabolic activation, the vascular microenvironment, or localized physical effects. These mechanisms cannot be replicated in standard in vitro culture systems. Therefore, these treatments are generally not suitable for conventional drug susceptibility testing and require more complex in vivo models (e.g., patient-derived xenograft, PDX models) or alternative assessment methods (e.g., genetic testing, immune microenvironment analysis) to predict efficacy.
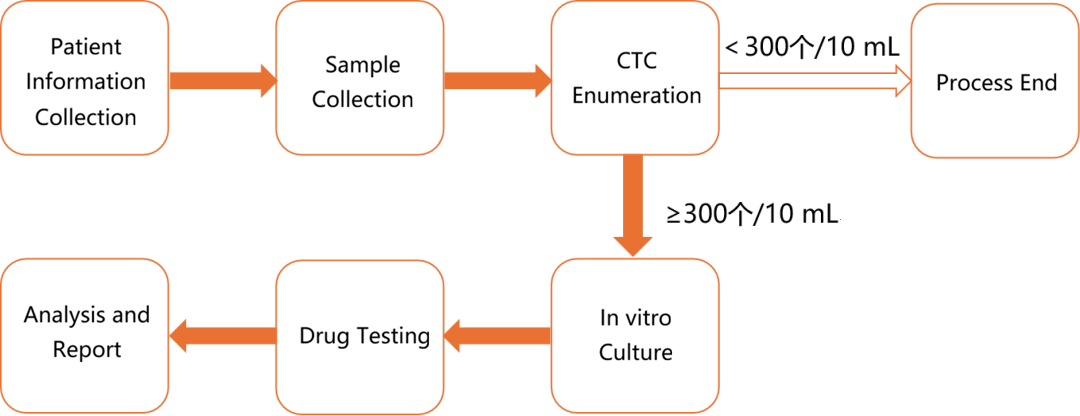
Q5: If I want to undergo drug susceptibility testing, what is the service process?
Q6: How much bodily fluid sample is needed for CTC culture?
At least 20 mL of blood, at least 50 mL of ascites, and the volume for other bodily fluids depends on the situation. Labyrinth has successfully achieved CTC culture from various bodily fluids, including pleural effusion, ascites, cerebrospinal fluid, peripheral blood, and bile.
Q7: How long does the entire drug susceptibility testing service process take?
CTC enumeration: 3 business days
In vitro culture: 15 business days
Drug testing and analysis: 15 business days
Q8: Is in vitro culture always successful?
Not necessarily. The success rate of in vitro culture depends on the cancer type, the individual patient's treatment stage, and the condition of the patient's cells. Labyrinth culture success rate is approximately 50%.
Q9: How many drugs can be tested in one drug susceptibility test?
The number of drugs is determined based on the in vitro culture outcome and the clinician's recommendations. Generally, the number of cells successfully cultured in vitro is sufficient to meet the requirements for drug testing.
Q10: What results does the drug susceptibility test report provide?
The report provides information on the sensitivity of the patient's CTCs to different drugs, aiding clinicians in determining a personalized treatment plan, effectively reducing ineffective medication use, and helping identify the optimal treatment strategy.
Q11: Can CTC-based drug susceptibility testing be repeated?
Yes. Tumors are heterogeneous diseases, and the molecular characteristics of tumor cells can change during disease progression and treatment, leading to drug resistance. CTC-based drug susceptibility testing can be repeated by collecting multiple blood samples during the treatment course for in vitro expansion, allowing real-time, dynamic monitoring of changes in drug sensitivity and providing a basis for adjusting treatment plans.
References
[1] Jiajla Tang, etc. CTC-derived pancreatic cancer models serve as research tools and are suitable for precision medicine approaches. Cell Rep Med, 2024 Aug 19:5(9):101692.